
Now that the Ebola virus has reached the United States, there is understandably a lot of panic about it. The news media certainly isn’t helping to put our minds at ease.
Ebola certainly is a scary disease, but even in Africa, it’s way down the list of causes of death.

Graphic courtesy of World Health Organization.
That’s not to say that Ebola is not a terrible and deadly disease — it is — but once we are reminded that it only spreads through direct contact with bodily fluids (including human waste), then we may be more able to be more rational about it.
One major advantage that we have in the United States that people in West African nations lack is modern sanitation. In its list of Ten Great Public Health Achievements in the 20th Century, the Centers for Disease Control and Prevention listed infectious disease control as a top achievement and improvements in sanitation and hygiene as crucial strategies.
Disease control resulted from improvements in sanitation and hygiene, the discovery of antibiotics, and the implementation of universal childhood vaccination programs….
The 19th century shift in population from country to city that accompanied industrialization and immigration led to overcrowding in poor housing served by inadequate or nonexistent public water supplies and waste-disposal systems. These conditions resulted in repeated outbreaks of cholera, dysentery, TB, typhoid fever, influenza, yellow fever, and malaria.
By 1900, however, the incidence of many of these diseases had begun to decline because of public health improvements, implementation of which continued into the 20th century. Local, state, and federal efforts to improve sanitation and hygiene reinforced the concept of collective “public health” action (e.g., to prevent infection by providing clean drinking water). By 1900, 40 of the 45 states had established health departments. The first county health departments were established in 1908. From the 1930s through the 1950s, state and local health departments made substantial progress in disease prevention activities, including sewage disposal, water treatment, food safety, organized solid waste disposal, and public education about hygienic practices (e.g., foodhandling and handwashing). Chlorination and other treatments of drinking water began in the early 1900s and became widespread public health practices, further decreasing the incidence of waterborne diseases. The incidence of TB also declined as improvements in housing reduced crowding and TB-control programs were initiated. In 1900, 194 of every 100,000 U.S. residents died from TB; most were residents of urban areas. In 1940 (before the introduction of antibiotic therapy), TB remained a leading cause of death, but the crude death rate had decreased to 46 per 100,000 persons.
U.S. Centers for Disease Control and Prevention
So that’s a reassuring feather in our cap when fighting Ebola here at home. But we can’t afford to get complacent about it.
Here in my home town of Indianapolis, we have a dirty little problem that nobody wanted to talk about for years. Storm drains that collect rainwater and dump it into waterways are commingled with sewer drains (this is known as a combined sewer system). So, whenever there’s a good rain, well you can probably guess the results.
Each year, the city of Indianapolis dumps between six and seven billion — that’s billion with a B! — gallons of raw, untreated waste into Eagle Creek, Fall Creek, Pleasant Run, Pogues Run and the White River.
Bob Segall, WTHR-TV Indianapolis
That’s a lot of raw sewage overflowing into our waterways where people boat, fish and occasionally swim. Indianapolis’s sewer system is more than 100 years old and simply doesn’t have enough capacity. Scary stuff, especially in light of the Ebola outbreak.
The good news is that help for my hometown is on the way. Because these conditions were a violation of the Clean Water Act, the U.S. Environmental Protection Agency sued the city, which led to a settlement and a Consent Decree for the city to fix the sewage system. Essentially, the city is only doing it because the feds are making them do it. Politicians don’t want to be responsible for massive increases in utility rates.
The city, along with Citizens Energy Group, the public utility that operates the water, sewer and natural gas systems in Indianapolis, is currently building a massive tunnel system to add capacity and minimize (notice I didn’t say eliminate) the overflows. The bad news is that it won’t be done until May 2016.
Indianapolis is far from alone in its challenges with an antiquated sewer system. According to the EPA, there are 213 large systems (each serving 50,000 or more people) nationwide with combined sewer overflows and 1,103 additional large systems with sanitary sewer overflows. The goal is to address all of them by the end of FY2016 — but it will take years beyond that for all of the necessary projects to be completed.

Graphic courtesy of the U.S. Environmental Protection Agency.

Graphic courtesy of the U.S. Environmental Protection Agency.
That’s why I find it totally incredulous that many voices within the GOP have proposed that we abolish the EPA altogether while simultaneously accusing the Obama administration of not being serious about protecting Americans from Ebola. Indeed, budget cuts have also hamstrung the CDC and the National Institutes of Health in their efforts to contain the disease and even develop a vaccine.
“NIH has been working on Ebola vaccines since 2001. It’s not like we suddenly woke up and thought, ‘Oh my gosh, we should have something ready here.’ Frankly, if we had not gone through our 10-year slide in research support, we probably would have had a vaccine in time for this that would’ve gone through clinical trials and would have been ready.”
Dr. Francis Collins, Director, National Institutes of Health
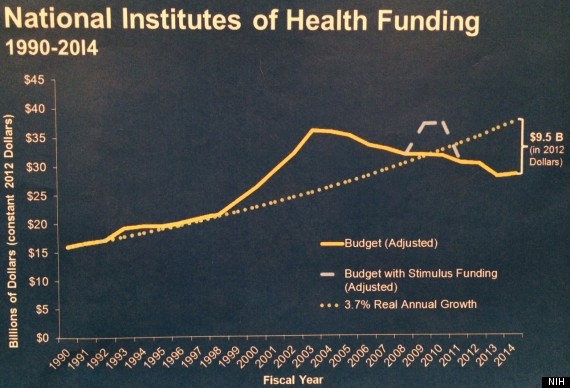
Graphic courtesy of National Institutes of Health.
